
Top navigation skipped

Health IT in TexasThe Doctor is … Online
Texas is a uniquely varied state, combining booming cities with thousands of square miles of countryside. And that represents a challenge for the medical field, and for people in need of medical care.
Despite fast growth in our cities, nearly 70 percent of Texas counties are considered rural, and according to the State Office of Rural Health, 64 of them lack a hospital; 25 do not have a single primary-care physician (Exhibit 1).
And Texas has a physician shortage. The state ranks 47th in the nation for its ratio of primary-care physicians per 100,000 people. In 2016, the U.S. Department of Health and Human Services estimated Texas would face a demand deficit of around 1,760 physicians by 2025, the second-largest gap among states (Exhibit 2).
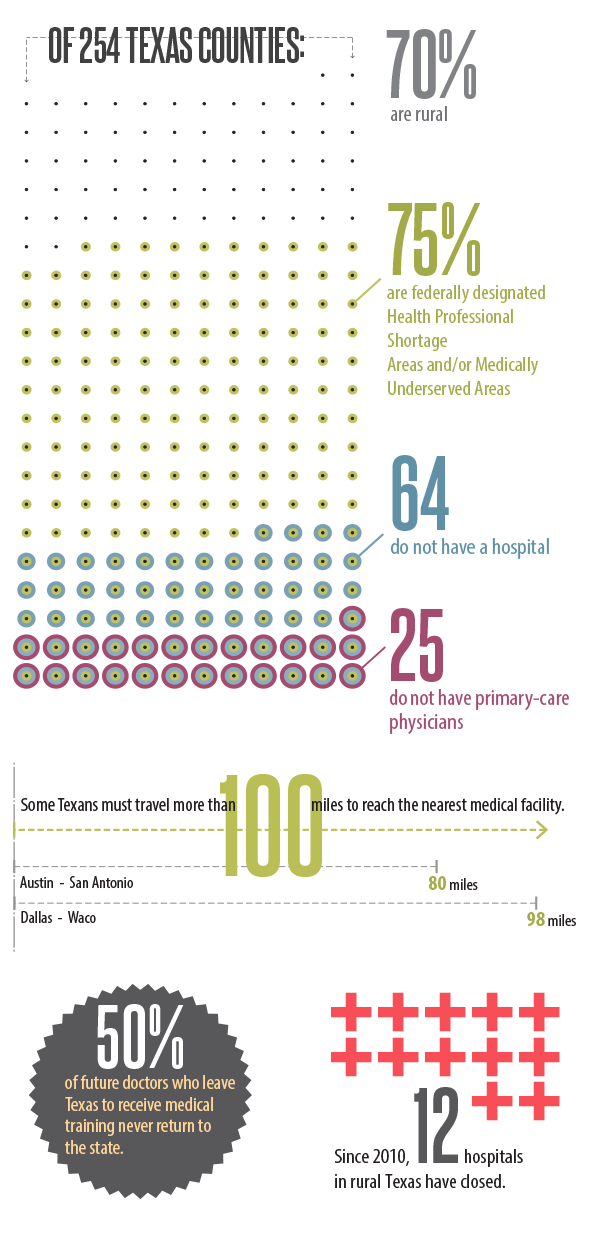
Exhibit 1: Fast Facts About Rural Health Care in Texas
Of 254 Texas Counties:
- 70% are rural
- 75% of Texas counties are federally designated Health Professional Shortage Areas and/or Medically Underserved Areas
- 64 Texas counties do not have a hospital
- 25 Texas counties do not have primary-care physicians
Some Texans must travel more than 100 miles to reach the nearest medical facility.
(Austin to San Antonio is 80 miles. Dallas to Waco is 98 miles.)
50% of future doctors who leave Texas to receive medical training never return to the state.
Since 2010, 12 hospitals in rural Texas have closed.
Sources: Texas Department of Agriculture, Texas State Office of Rural Health
Exhibit 2: Projected Deficit/surplus of Physicians, 2025
| Category | Deficit or Surplus of Physicians by 2025 |
|---|---|
| Florida | -3,060 |
| Texas | -1,760 |
| California | -1,550 |
| Georgia | -1,310 |
| Missouri | -1,220 |
| Ohio | -1,200 |
| Alabama | -1,190 |
| Indiana | -1,180 |
| New Jersey | -1,060 |
| Tennessee | -1,050 |
| Alaska | 80 |
| Hawaii | 80 |
| New York | 120 |
| Vermont | 120 |
| Oregon | 130 |
| Colorado | 160 |
| Maine | 220 |
| Maryland | 240 |
| Minnesota | 300 |
| Massachusetts | 890 |
Note: Estimated differences equal supply minus demand; a negative difference reflects a shortage (i.e., supply less than demand), while a positive difference indicates a surplus (i.e., supply greater than demand).
Sources: U.S. Department of Health and Human Services, Health Resources and Services Administration
Health information technology (health IT) is a promising approach for tackling Texas health care challenges, particularly in its vast but sparsely populated rural areas. Health IT includes a variety of services, generally defined as:
- telemedicine: health care delivered by a physician through the web, videoconferencing and other technologies, including remote reviews of patient records such as X-rays.
- telehealth: a broader term encompassing telemedicine as well as remote health care delivered by other health professionals, such as nurses and pharmacists, and services such as professional and public health education.
- telemonitoring: use of monitoring equipment, such as blood pressure devices or pacemakers, which transmit data to a physician.
Thanks to new laws passed in the 2017 regular legislative session, these services may gain broader reach in Texas.